
Patient-Centered Clinic Design
Employer
Client
Location
Timeline
My role
Team
Independent consultancy / master's thesis
Correctional Health Services, NYCHHC
New York, New York
14 months
Project manager, design co-lead
Team of 1 additional designer / grad student
With New York City's plans to move the location of jails on Rikers Island, the administration of Correctional Health Services would be asked to submit requests for the design of clinics in future facilities.
To help the organization prepare, I spent a year learning about the current clinic spaces: observing process flows, mapping the layouts, interviewing patients and providers, and facilitating user-led paper prototyping of new clinic designs.
The project's final deliverable was a comprehensive new clinic floor plan that solved for unmet needs and pain points - aimed at decreasing barriers to care, increasing patient engagement with services, and ultimately improving health outcomes. The project was also part of my graduate thesis in social impact design.

The one-and-only photo I took onsite (at a location that is open to visitors) - no phones or cameras were permitted inside the facilities.
Project summary
The problem:

A common clinic "waiting room"
Context & constraints:
-
Rigid environment: Tightly controlled, high stakes, resource-limited environment with limited procedural flexibility.
-
Opposing stakeholders: Three primary stakeholder groups with discrete and sometimes opposing needs (groups: healthcare providers, people who are detained, and corrections officers).
-
IRB approval: Because people who are detained in correctional facilities are classified as vulnerable populations, extensive approval by an official academic ethics committee was required for any research.
Barriers to care: People who were detained New York's jails faced significant barriers to care, despite on-site comprehensive services that were currently provided inside all of the the facilities.
Project goal - to solve for:
How might the spatial design of healthcare clinics inside New York City's jails decrease barriers to care?
Process steps
-
Needs assessment: Performed mixed-methods, primary on-site research with patients and providers to illuminate unseen challenges (IRB approval required).
-
Data analysis and insights: Discovered that current clinic designs created cross-cutting barriers to care.
-
Project scoping with administration: Facilitated 2 workshops for five members of Correctional Health Services upper administration and clinical leadership, wherein we presented findings and collaboratively determined the project's focus.
-
User-led prototyping: Facilitated paper prototyping with patients and providers, identifying new ways to better meet their needs.
-
Secondary research: Performed a landscape analysis of human-centered design in architecture, interviewed external subject-matter experts, and researched current 'best practices' in correctional healthcare clinic design (scant work exists worldwide).
-
Final deliverable: Produced an innovative new clinic design and design principles to guide the construction of new facilities.
-
Monitoring & evaluation: Created a comprehensive M&E plan based on a Theory of Change framework, with defined variables, measurement guidelines, and a timeline.
_edited_edited.jpg)
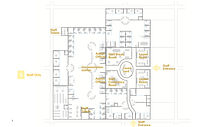
Diagram of a clinic layout and patient care process flows therein - with special attention to pain points and inefficiencies.
Solution & impact:
We delivered a novel health clinic design and a set of specific design principles to the organization's administration, that would be used to guide planning of new facilities.

Innovative clinic design with numerous improvements
Wins, losses, learnings:
-
Surprising win: xxxy
-
Unexpected hurdle: xxx
-
With more ______ we would have... xxx.
-
Most valuable learning: xx




A new layout designed by a clinic manager.
Design process deep dive.
1
Needs assessment:
Rightly so, although at first I was surprised that this included activities like paper prototyping to co-design new clinics. The process of acquiring approval sparked what has become an interest and concern in my career: the lack of consistent ethics guidelines in design research. )
Performed mixed-methods, primary on-site research with patients and providers to illuminate unseen challenges (IRB approval required)
My on-site interviews with patients and providers, and facilitation of collaborative systems mapping revealed that clinic designs create significant barriers to care.
.jpg)
During a thorough clinic tour, I map spatial challenges and pain points.
Performed mixed-methods, primary on-site research with patients and providers to illuminate unseen challenges (IRB approval required)
Research methodology:
-
On-site observation
-
Intercept, structured + semi-structured interviews
-
Problem mapping workshops
-
Focus groups / generative sessions with clinical staff
-
Collaborative spatial and process mapping with clinical health clinic managers
_edited_edited.jpg)


Classes took place in an unused ICU room







Classes took place in an unused ICU room





3
Project scoping:
xxx
-
xxx
-
A
[ visual coming soon ]
4
User-led prototyping:
xxx
-
xxx
-
A
Facilitated paper prototyping with patients and providers, identifying new ways to better meet their needs.
Performed a landscape analysis of human-centered design in architecture, interviewed external subject-matter experts, and researched current 'best practices' in correctional healthcare clinic design (scant work exists worldwide).
5
Secondary research:
xxx
-
xxx
-
A









[ visual coming soon ]
6
Final deliverable & impact:
xxx
-
xxx
-
A

























[ visual coming soon ]
7
Monitoring & evaluation:
xxx
-
xxx
-
A
Created a comprehensive M&E plan based on a Theory of Change framework, with defined variables, measurement guidelines, and a timeline.
An innovative clinic design that contains numerous improvements.

A patient access care easily, meeting his needs and organizational goals.
Challenge
No guarantee of career advancement: Nurses would need to devote many hours each week to training, but the undertaking might not yield tangible value.
Solutions
National endorsement: We were able to secure endorsement from the University of Rwanda.
Minimized time commitment: With support from the ICU medical director, we were able to hold the course in an extra room in the ICU, enabling nurses to attend it during their work hours.
Impact
Unified participation: Official backing from a high level institution provided incentivizing explicit value, and immediately accessible classes resulted in every ICU nurse deciding to take the course.
2
Data analysis & insights:
Analysis and synthesis methodology:
-
Customer journey and service blueprint mapping
-
Process diagrams in the context of clinic layout and spatial design
-
Affinity mapping to reveal consistent themes
-
Discovered that current clinic designs created cross-cutting barriers to care.
Produced an innovative new clinic design and design principles to guide the construction of new facilities.
I created a prototyping tool to explore pain points and goals with patients and providers, with which they could design new health clinics to better meet their needs.
A patient creates a new health clinic that would better meet his needs.
talk about how this played out w spatial design - a few examples?